The batch failed again.
The operators followed the procedure. The equipment was calibrated. The raw materials passed incoming QC. And yet the critical quality attributes came back out of specification — for the third time in two production campaigns.
This is not an unusual story. Across pharmaceutical manufacturing, batch rejection events that resist conventional investigation are far more common than most organisations publicly admit. The financial consequences are immediate: discarded materials, lost reactor time, rescheduled campaigns. The strategic consequences take longer to surface — degraded client confidence, unreliable production planning, and a cost structure that quietly makes certain programmes uncompetitive.
The question most teams eventually face is not whether to fix it. It is whether their current tools are actually capable of finding what went wrong.
Right first time: what it actually means
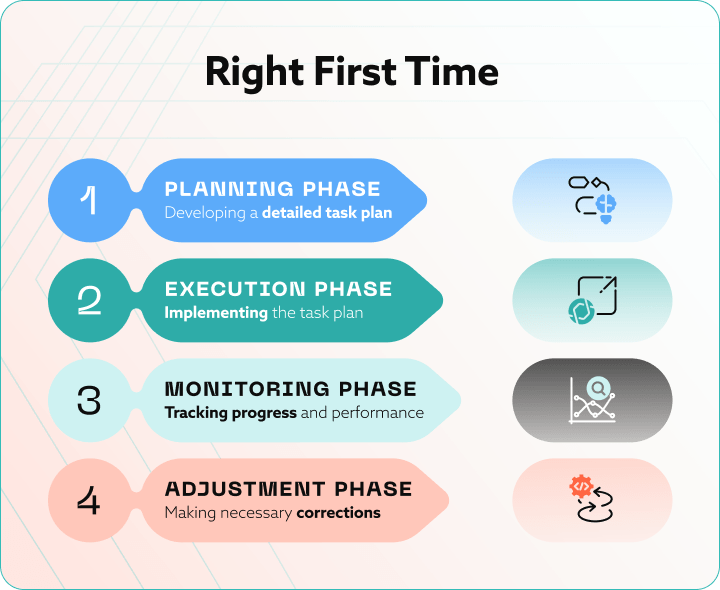
Right first time (RFT) manufacturing is the discipline of producing product that meets all GMP quality specifications from the first execution, without rework, reprocessing, or rejection. For multi-stage processes — which describes virtually every pharmaceutical manufacturing operation — RFT is calculated across each stage, meaning a single weak point pulls down the entire campaign score.
In pharmaceutical manufacturing, the stakes of a failed batch go beyond lost production time. A rejected batch means discarded active pharmaceutical ingredient, regulatory deviation documentation, potential supply disruption, and, in persistent cases, questions about the reliability of the entire programme.
Typical RFT baselines vary by manufacturing context, as shown below.
|
Manufacturing context |
Typical RFT baseline |
Improvement target |
Primary failure driver |
|
General Manufacturing |
85–92% |
>95% |
Equipment variance, operator error |
|
Pharmaceutical — Solid Dose |
88–94% |
>97% |
Parameter interdependencies, material variability |
|
Small-Molecule API / Drug Substance |
80–92% |
>96% |
Multivariate process complexity, PSD, crystallisation |
|
Biologics / Bioprocess |
75–88% |
>94% |
Cell culture variability, upstream–downstream coupling |
GlaxoSmithKline has documented batch rejection rates dropping from 5.2% to 0.8% within eight monthsfollowing structured RFT improvement initiatives. The gap between those two numbers reflects both the scale of the problem and what deliberate intervention can produce.
What most pharmaceutical manufacturers have not yet confronted is that general manufacturing improvement logic does not translate cleanly to pharmaceutical process complexity. The methods were developed for a different class of problem.
When the investigation runs out of answers
There is a diagnostic assumption embedded in most pharmaceutical deviation management systems: if a batch fails, something went wrong in its execution. An operator made a judgment call. A parameter drifted past its setpoint. A piece of equipment behaved unexpectedly.
This assumption holds for a significant portion of failures. But for a specific category — recurrent, non-random, and stubbornly inconclusive after investigation — it is the wrong frame entirely.
These failures are not execution failures. They are complexity failures. The process is operating exactly as designed. The problem is that the design does not adequately capture the full interaction space of variables determining the outcome. Adjusting the obvious parameters improves one critical quality attribute and worsens another. The investigation closes without a definitive cause. The next campaign runs. The problem returns.
A pharmaceutical manufacturer encountered precisely this pattern in its small-molecule drug substance operations. Despite experienced operators, established procedures, and a functioning deviation management programme, the organisation faced recurrent production delays, frequent batch rejections, and unstable campaigns. The core issue was repeated out-of-specification results in critical quality attributes during chemical reactor operations. Over time, these failures translated into multi-million-euro annual losses driven by discarded material, lost production time, and cascading inefficiencies across the manufacturing network.
If your investigation cycle keeps closing without a definitive root cause, the problem is not the investigation. It is that the failure mechanism is multivariate and the tools being applied are univariate.
Further reading: cGMP Deviations in Pharmaceuticals: The Full Guide
Why pharmaceutical processes are particularly difficult
Pharmaceutical manufacturing is a sequence of tightly coupled chemical and physical operations — reaction kinetics, heat and mass transfer, solvent interactions, solid-liquid transformations — where small variations at one stage can propagate into significantly altered outcomes several stages downstream.
Crystal formation behaviour, particle morphology, and purification efficiency are all sensitive to interdependent process parameters, many of which cannot be meaningfully evaluated in isolation. The same parameter setting that is optimal under one combination of upstream conditions may be problematic under a different combination that appears, on paper, identical.
In the case described here, the primary hidden culprits were particle size distribution (PSD) and sedimentation behaviour — two quality-relevant physical phenomena whose effects were not only significant individually but actively competing. Adjustments that improved PSD outcomes worsened sedimentation variability. Adjustments targeting sedimentation introduced instability in PSD. The deviations were subtle, cumulative, and highly context-dependent, which is precisely why statistical process control and traditional univariate analysis could not capture the interaction effects driving the failures.
The result was a cycle familiar to anyone who has managed a complex pharmaceutical programme: undetected process drift, late-stage out-of-specification results, batch losses, and an investigation process that consistently exhausted its explanatory power before finding the root cause.
The limits of conventional root cause analysis
Conventional investigation methods are built for a world where failures have discrete, identifiable causes. One parameter goes out of range. One piece of equipment malfunctions. One incoming material lot has an anomalous characteristic. Identify the cause, correct it, close the CAPA.
This model fails when the failure mechanism is multivariate — when too many critical process parameters are influencing the outcome simultaneously, when the relationships between variables are non-linear and time-dependent, and when historical batch data exists but sits siloed across separate systems: process historians, LIMS, batch records, equipment logs, never integrated into a form that allows cross-variable analysis.
A 2025 review in the International Journal of Pharmaceutics addresses this directly: pharmaceutical manufacturing’s transition to advanced quality control requires predictive adaptive modelling and real-time process optimisation precisely because human interpretation cannot scale to the full complexity of modern process data. The data is there. The patterns are there. But they are invisible to the tools most organisations are still using.
The process capability index may tell you a process is drifting. It will not tell you which combination of upstream conditions is creating the drift. That question is not answerable through more thorough manual investigation. It requires a different analytical method.
Further reading: How to automate GMP compliance and CAPA management
What digitalization actually means in this context
Digitalization in pharmaceutical manufacturing is often discussed in vague terms. In the specific context of batch quality, it means something concrete: the ability to integrate data from across the full process lifecycle and evaluate it simultaneously, at a level of complexity that manual analysis cannot reach. BGO Software’s overview of digital transformation in pharma outlines how this integration works end to end.
What gets integrated is broader than most teams initially expect. Raw material attributes. Batch execution records. Reactor conditions — temperature, pressure, agitation, timing. Media addition volumes and sequences. Storage and hold conditions. Downstream purification parameters. Each of these data streams, individually, tells a partial story. Integrated and evaluated together, they reveal patterns and interactions invisible in any single stream.
Three capabilities separate this approach from conventional analysis:
|
Capability |
Traditional analysis |
Digital process intelligence |
|
Variable evaluation |
One parameter at a time (univariate) |
Hundreds of parameters simultaneously (multivariate) |
|
Deviation detection |
Post-failure, after CQA is already out of spec |
Pre-failure, from early in-process signals |
|
Process targets |
Fixed setpoints |
Optimal operating ranges under real variation |
|
Data integration |
Siloed — LIMS, historians, batch records separate |
Unified across the full process lifecycle |
|
Investigation speed |
Days to weeks per CAPA cycle |
Real-time, continuous monitoring |
|
Regulatory alignment |
Compliance-driven, end-product testing |
ICH Q8/Q9/Q10 process understanding framework |
Multivariate evaluation assesses combinations of conditions across hundreds of parameters simultaneously — identifying interaction effects that univariate methods structurally cannot detect. This is the operational basis of Quality by Design at scale.
Early deviation detection means predictive models identify signals of process drift before critical quality attributes are compromised. The intervention point shifts from reactive investigation to proactive correction. BGO’s article on real-time process support and predictive analytics in GMP manufacturing covers how this works in practice under GMP constraints.
Optimal operating ranges replace fixed setpoints. Real processes behave under variation, and the most useful output is not a single target value but a defined window of conditions within which quality outcomes are reliably achieved. This is precisely what ICH Q8, Q9, and Q10 require as evidence of genuine process understanding.
In practice, this is often implemented through Process Analytical Technology (PAT) frameworks and Manufacturing Execution System integration — combining real-time data capture with the analytical models needed to interpret it. The result is a continuous process verification capability that turns historical batch data into predictive intelligence, rather than a post-failure audit trail.
What the data revealed
The analytical platform applied to the failing programme integrated data from every stage: raw material attributes, batch execution records, reactor conditions, media additions, storage and hold conditions, downstream purification steps. Rather than searching for a single root cause, the system evaluated patterns, interactions, and correlations across the full dataset at once.
What it found was not a single failure point. It was a map of conditions previously invisible because they only became problematic in specific combinations — that reliably predicted deviation risk in the critical quality attributes. The parameters influencing PSD and sedimentation were identified. The combinations of conditions that amplified deviation risk were quantified. Optimal operating ranges were defined that accounted for the interdependency between the two phenomena, rather than optimising each in isolation.
Predictive models then recommended optimal temperature profiles, refined the timing and volumes of process additions, and monitored batches in near real time against risk-based thresholds. The intervention point moved from post-failure investigation to in-process monitoring. Instead of discovering that a batch had failed, the process team was alerted to conditions predicting a failure — early enough to act.
This is not an incremental improvement on conventional deviation management. It is a different operating model: from expert intuition to evidence-based decision-making, from reactive investigation to predictive control.
Further reading: BGO’s GMP validated systems and manufacturing intelligence platform
The results
Following implementation, the outcomes were measurable across every dimension that matters to pharmaceutical manufacturing operations.
|
Metric |
Before implementation |
After implementation |
|
Production campaign stability |
Unstable — recurrent batch rejections |
Most stable campaign to date |
|
Right first time batch execution |
Below target, unpredictable |
Substantially increased |
|
Batch-to-batch variability |
High, context-dependent |
Dramatically reduced across runs |
|
Deviation detection point |
Post-failure (end of campaign review) |
In-process (before CQA is compromised) |
|
Production planning confidence |
Low — unreliable client commitments |
High — reliable supply commitments |
|
Process understanding basis |
Expert intuition |
Evidence-based, data-driven |
|
Foundation for improvement |
Programme-specific, not transferable |
Scalable process intelligence framework |
Beyond the immediate operational gains, the organisation acquired something with longer-term value: a data-driven understanding of how the process actually behaves, not how it was assumed to behave. The ability to forecast deviation risk early. A foundation for continuous improvement applicable not just to this programme but to future campaigns with similar process characteristics.
A 2025 study in the European Journal of Pharmaceutical Sciences found that machine learning-based optimisation of API continuous manufacturing produced solutions averaging 58% better than standard sampling approaches. The multi-million-euro annual losses in the case described here did not stop because someone found the root cause of one batch failure. They stopped recurring because the organisation understood the process well enough to prevent failures from forming.
Why this has become a commercial issue
For pharmaceutical manufacturers operating under increasing cost pressure and growing regulatory scrutiny, RFT rate has moved beyond being a quality metric. It is now part of how manufacturing partners are evaluated.
Clients selecting partners for complex programmes are asking different questions than they were five years ago. Not just whether the equipment and regulatory track record are in order — but what the process understanding actually is, how batch variability is managed, and what happens when conventional investigation tools run out of answers. For CDMOs in particular, this shift is reshaping how partnerships are structured: BGO’s analysis of CDMO trends in 2025shows how process capability has moved from a differentiator to a baseline expectation.
The cost of poor quality in pharmaceutical manufacturing — spanning failed batch losses, deviation investigation time, regulatory submissions, and supply disruption — is routinely underestimated until it becomes unavoidable. Organisations that have invested in process intelligence are building a position reflected in every metric that clients track: batch yield, campaign stability, deviation closure timelines, technology transfer speed.
The regulatory dimension is tightening in parallel. The 2023 revision of EU GMP Annex 1 shifted the evidentiary standard from proving rule compliance to demonstrating that manufacturing is continuously in control — a requirement that fragmented, siloed data systems structurally cannot meet. The gap between organisations investing in process intelligence and those that are not is widening.
The practical implication
If your programmes are experiencing recurrent batch variability that conventional root cause analysis has not resolved, the limiting factor is almost certainly not effort or expertise. It is the analytical method being applied to a problem that requires a different approach.
The data needed to solve the problem already exists in most manufacturing organisations. It sits in process historians, LIMS, batch records, and equipment logs. The technology to integrate and evaluate it is available. The regulatory framework supports it. The commercial case, measured in avoided batch losses and improved campaign performance, is direct.
The organisations achieving consistently high RFT rates are not doing so because their processes are simpler. They are doing so because they understand their processes more completely — and because they built that understanding with tools suited to the actual complexity of the problem.
Ready to assess what this looks like for your specific programme? Speak with our process team.
References
- Rezaeizadeh M, Razavi SM, Muzzio FJ. Current state of machine learning implementation in pharmaceutical process modeling for oral solid dosage forms. Int J Pharm. 2025. [Link]
- Wu KE, Brown CJ, et al. Testing on continuous production of mefenamic acids — Design of experiment through simulation and process optimisation. Eur J Pharm Sci. 2025. [Link]

Healthcare business analyst with expertise in marketing and business development, and holds an MPharm degree. He specialises in creating and executing communication strategies that make digital health solutions and pharmaceutical technologies clear, accessible, and resonation for their audiences.
link to the author’s linkedin profile